Answer Summary
DME providers maximize cash flow by segmenting accounts receivable based on payer behavior and recovery probability, ensuring staff effort is directed toward high-value claims that stabilize working capital. As the industry faces a 5.84% growth in unit costs and a 2.5% “efficiency adjustment” reduction in work RVUs in 2026, organizations must target a Days Sales Outstanding (DSO) in the mid-40 to mid-50 range to offset tightening margins. By shifting from reactive aging-bucket follow-ups to predictive intelligence, providers can shorten the revenue cycle and maintain the liquidity necessary to navigate increasing payer volatility.
Introduction: Why Cash Flow Became the Real Performance Metric
For years, DME providers measured success by billed revenue. Growth targets, referral volume, and claim submission counts dominated performance discussions. Cash flow—while important—was often treated as a lagging outcome that would resolve itself if billing stayed strong.
In 2026, that assumption no longer holds.
Providers across the industry are discovering that strong billing does not guarantee usable cash. Payment delays, increased denial activity, and payer-specific variability have widened the gap between services rendered and revenue realized. Organizations with impressive top-line numbers still struggle to meet payroll, fund inventory, or invest in growth.
Cash flow has become the true performance metric—not because revenue matters less, but because timing and predictability matter more. Accounts receivable is no longer a back-office function. It is the control system that determines whether revenue becomes working capital.
How Cash Flow Breaks Down in the DME Revenue Cycle
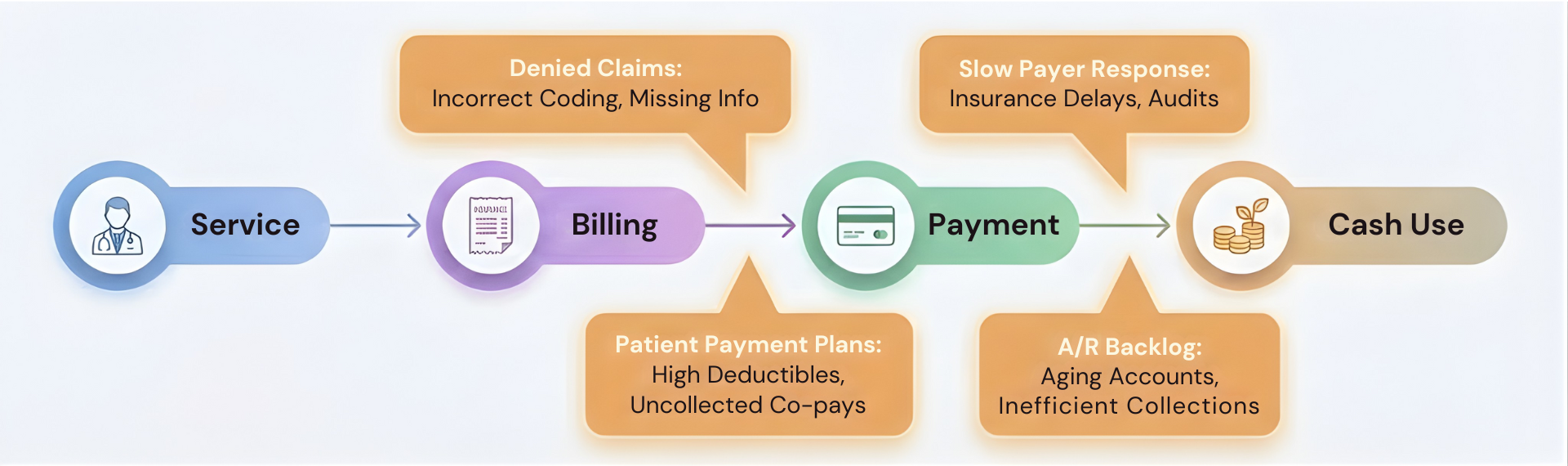
To improve cash flow, providers must first understand where it breaks.
The DME revenue cycle includes multiple handoffs between departments and systems:
- Intake and qualification
- Documentation collection
- Authorization and eligibility
- Delivery
- Claim submission
- Payer adjudication
- Payment, denial, or delay
Cash stalls when any link in this chain weakens. The most common breakdowns include incomplete documentation, authorization mismatches, and denials that require rework. Each delay compounds the next, stretching the time between service and payment.
Traditional metrics like average days in A/R often obscure these realities. Averages hide variability and fail to reveal where cash is actually getting stuck. Providers need to look beyond surface metrics to regain control.
A/R Segmentation: Treating All Dollars Differently
One of the most common A/R mistakes is treating all receivables the same. Not all dollars carry equal risk or recovery potential.
Effective providers segment A/R based on:
- Payer behavior
- Claim type
- Dollar value
- Likelihood of recovery
High-risk claims require proactive attention. Low-risk claims often resolve without intensive follow-up. Applying equal effort to both wastes resources and slows cash velocity.
Segmentation allows providers to direct staff time where it produces the greatest return. This shift alone often reduces A/R aging without increasing workload.
Intake and Documentation as Cash-Flow Controls
Cash flow problems often originate far upstream from A/R.
Incomplete intake, inconsistent documentation standards, and weak medical necessity narratives create claims that are technically billable but practically delayed. These claims move into A/R already compromised.
Strong providers treat intake and documentation as cash-flow controls, not administrative tasks. They ensure:
- Documentation requirements are enforced consistently
- Incomplete records do not advance downstream
- Medical necessity is substantiated clearly
By preventing weak claims from entering the system, providers reduce downstream rework and accelerate payment.
Authorization and Eligibility Discipline
Authorization failures remain one of the most preventable causes of delayed or lost revenue.
Common issues include:
- Expired authorizations
- Mismatches between authorized and delivered items
- Eligibility changes not identified before delivery
Each error creates delivered-but-unbillable equipment—a direct cash-flow drain.
Providers that stabilize cash flow align delivery decisions with billing readiness. Authorization and eligibility are verified continuously, not just at intake. This discipline protects revenue before it reaches A/R.
Denial Prevention as a Cash Strategy
Denial management is often framed as a recovery function. In reality, denial prevention is one of the most effective cash-flow strategies available.
Appeals are expensive. They require staff time, extend payment timelines, and often recover only a portion of the original claim value. Prevention avoids these costs entirely.
Providers that analyze denial patterns and feed insights back into workflows see measurable improvements in:
- First-pass claim acceptance
- Payment timing
- Staff productivity
Reducing denial volume stabilizes cash by shortening the revenue cycle—not by increasing activity.
A/R Follow-Up That Improves Cash, Not Activity
Traditional A/R models reward activity: calls made, notes logged, accounts touched. These metrics create the illusion of progress without guaranteeing results.
Cash-focused A/R management prioritizes:
- Claims with high recovery probability
- Time-sensitive balances
- High-dollar exposure
Low-probability claims are worked strategically or written off intentionally. This approach reduces wasted effort and improves overall cash realization.
More follow-up does not equal more cash. Smarter follow-up does.
Measuring Cash-Flow Health the Right Way
Cash flow cannot be managed with lagging indicators alone.
Providers should monitor:
- Payment timing variance
- First-pass claim acceptance rates
- Resolution velocity by payer
- Percentage of A/R requiring escalation
These metrics reveal whether workflows are stable and predictable. When variance increases, cash risk follows.
Leadership teams that rely solely on high-level financial statements often react too late. Operational metrics provide early warning.
Financial Forecasting Using A/R Intelligence
Forecasting based on historical averages is increasingly unreliable. Payer behavior shifts, authorization programs expand, and reimbursement policies evolve.
Advanced providers use A/R intelligence to forecast cash flow dynamically. By analyzing payer-specific timing and claim characteristics, they can:
- Anticipate cash shortfalls
- Adjust purchasing and staffing
- Avoid reactive decision-making
Predictive forecasting turns A/R from a reporting function into a planning asset.
Technology’s Role in Cash-Flow Optimization
Technology can strengthen cash-flow control—but only when applied deliberately.
Automation helps by:
- Enforcing documentation standards
- Prioritizing A/R work intelligently
- Improving visibility across departments
It creates risk when:
- Poor workflows are automated
- Exceptions lack oversight
- Outputs are not monitored
Under 42 CFR § 424.57, suppliers remain accountable regardless of automation. Governance must accompany technology to protect compliance and financial integrity.
Common Cash-Flow Mistakes DME Providers Make
Providers undermine cash flow when they:
- Chase volume without assessing collectability
- Ignore payer-specific payment behavior
- Treat A/R as a back-office problem
- Delay addressing documentation weaknesses
Each mistake compounds timing risk. Cash flow improves when providers address root causes rather than symptoms.
How Wonder Worth Solutions Helps Stabilize Cash Flow
Wonder Worth Solutions works with DME providers to assess A/R workflow maturity, identify cash-flow risk drivers, and design prioritization frameworks that convert revenue into usable cash more reliably.
The goal is not more billing but more predictability.
Conclusion: Cash Flow Is Engineered, Not Hoped For
In 2026, cash flow stability separates resilient DME providers from reactive ones. Strong revenue means little if payment timing is unpredictable and A/R workflows lack control.
Providers that segment receivables, enforce upstream discipline, prevent denials, and prioritize effort intelligently transform A/R into a strategic asset. Cash flow becomes predictable—not by chance, but by design.