
Introduction:
Inaccurate auditing documentation can lead to compliance issues, claim denials, and operational inefficiencies—problems no DME provider can afford. Regular audits of your documentation processes ensure your records are accurate, complete, and compliant with regulatory requirements.
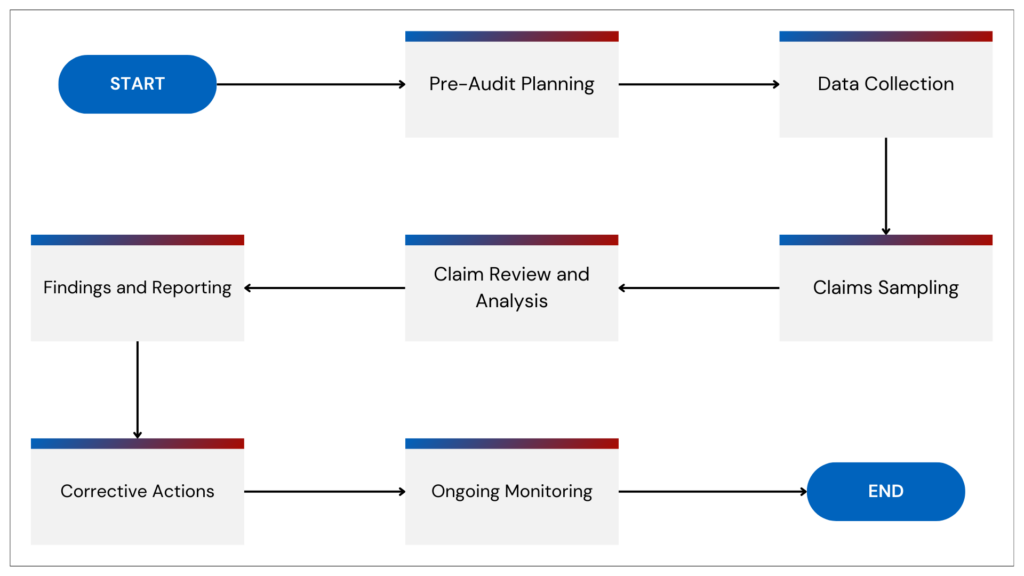
This blog outlines a step-by-step guide to auditing your DME documentation workflows, helping you identify gaps, correct errors, and streamline operations for long-term success.
Why Documentation Audits Are Essential
- Ensure Compliance:
- Accurate documentation helps avoid penalties from regulatory bodies like CMS.
- Reduce Claim Denials:
- Errors or missing information are common reasons for claim rejections.
- Streamline Workflows:
- Identifying bottlenecks improves efficiency and reduces staff workload.
- Build Trust with Stakeholders:
- Reliable documentation enhances relationships with patients, payers, and regulators.
Step-by-Step Guide to Auditing Your Documentation Processes
1. Define the Scope of Your Audit
- Why It’s Important: Focused audits are more effective and less disruptive to daily operations.
- How to Do It:
- Decide whether to review all documentation or target specific areas, such as claims, patient intake, or inventory records.
- Set clear objectives, like improving claim accuracy or reducing documentation errors.
2. Gather and Organize Records
- Why It’s Important: Consolidating records ensures a thorough and accurate review.
- How to Do It:
- Use electronic health records (EHR) or document management software to compile all relevant files.
- Categorize documents by type (e.g., insurance forms, care plans, equipment logs) for easier analysis.
3. Review Documentation Against Standards
- Why It’s Important: Comparing records to regulatory and payer requirements ensures compliance.
- How to Do It:
- Cross-check patient records, claims, and reports with CMS and payer guidelines.
- Use audit templates or checklists to streamline the process.
4. Identify Errors and Gaps
- Why It’s Important: Pinpointing issues allows for targeted corrections.
- How to Do It:
- Look for incomplete fields, missing signatures, or outdated forms.
- Use analytics tools to identify recurring issues like incorrect coding or delayed submissions.
5. Implement Corrective Actions
- Why It’s Important: Fixing errors promptly reduces risk and prevents future problems.
- How to Do It:
- Update policies and train staff on documentation best practices.
- Automate error-prone tasks like claims submission or patient intake.
6. Establish a Continuous Audit Cycle
- Why It’s Important: Regular audits ensure long-term accuracy and compliance.
- How to Do It:
- Schedule quarterly or biannual audits to catch and resolve issues early.
- Assign a dedicated compliance officer or team to oversee the process.
Common Errors Found During Documentation Audits
- Incomplete Records: Missing patient information or required signatures.
- Coding Errors: Incorrect billing codes leading to claim denials.
- Outdated Templates: Using forms that don’t meet current payer or regulatory requirements.
- Manual Entry Mistakes: Typos or data entry errors in critical fields.
Real-World Benefits of Documentation Audits
DME providers who conduct regular audits report:
- 35% Fewer Claim Denials: Accurate records streamline the approval process.
- 30% Time Savings: Improved workflows reduce staff time spent on corrections.
- 20% Higher Compliance Rates: Regular reviews ensure records meet evolving standards.
WWS Value Proposition
At WWS, we help DME providers enhance documentation accuracy with:
- Audit Templates and Checklists: Simplify the review process with proven tools.
- Automation Solutions: Reduce manual errors in claims and patient records.
- Training Programs: Equip staff with best practices for compliant documentation.
Partner with WWS to streamline your documentation workflows and improve operational efficiency.

