Answer Summary
DME providers integrate telehealth by embedding virtual interactions directly into intake, qualification, and follow-up workflows to compress care cycles and reduce administrative friction. This strategy is essential as the 2026 Medicare Physician Fee Schedule introduces stricter “virtual presence” supervision rules and a mandatory transition for many practitioners to list specific service locations, which can increase administrative costs by up to $1 million for large systems. By operationalizing these virtual touchpoints, providers can achieve a 30% reduction in intake cycle times while maintaining the rigorous documentation standards required for CMS compliance.
Introduction: Telehealth as an Operational Lever, Not a Convenience Feature
Telehealth adoption among DME providers accelerated rapidly over the past several years. While many organizations initially implemented virtual tools to address access challenges, fewer took the next step: integrating telehealth directly into operational and revenue-cycle workflows.
This case study highlights how a mid-sized home medical equipment (HME) provider moved beyond ad hoc virtual visits and intentionally embedded telehealth into intake, documentation, and follow-up processes. The result was improved efficiency, reduced operational friction, and a measurable increase in patient satisfaction—without compromising compliance or billing accuracy.
Provider Background
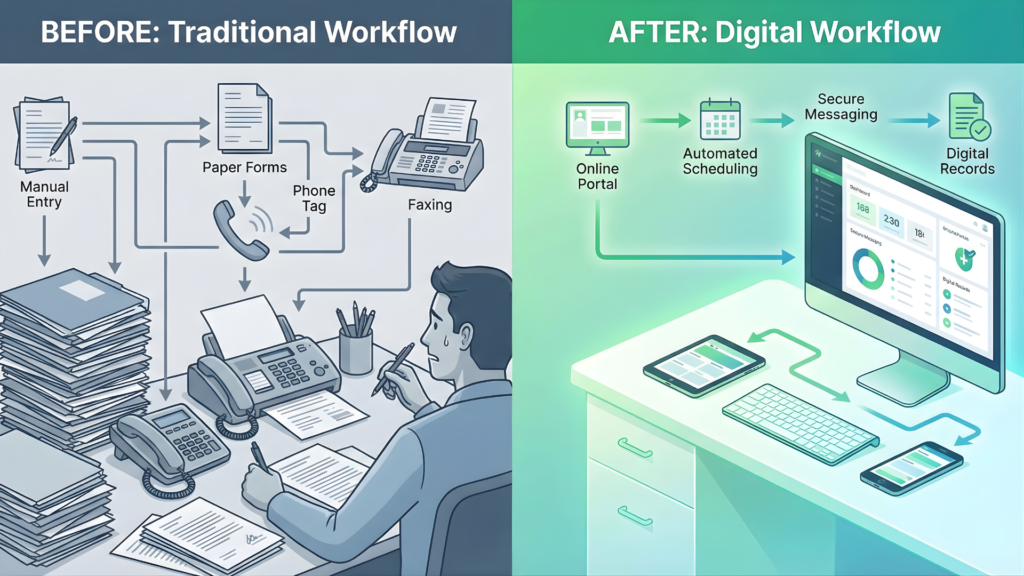
The provider featured in this case study operates across multiple service areas, offering respiratory equipment, mobility devices, and home medical supplies. Prior to telehealth integration, the organization relied heavily on phone-based intake, in-person follow-ups, and manual documentation reconciliation.
Key challenges included:
- High intake cycle times
- Frequent documentation rework
- Missed or delayed follow-up appointments
- Increasing staff workload without proportional revenue gains
Leadership recognized that telehealth could help—but only if it was implemented as part of a broader workflow redesign.
The Challenge: Fragmented Patient Interactions and Workflow Delays
Before integration, telehealth was used inconsistently. Some staff conducted virtual check-ins, while others relied solely on phone calls or in-person visits. Documentation from these interactions often lived outside core systems, requiring manual entry later.
This fragmentation created several issues:
- Incomplete or delayed documentation
- Multiple patient touchpoints for the same issue
- Increased risk of billing delays or denials
- Frustration for both staff and patients
Telehealth existed—but it was not operationalized.
The Approach: Integrating Telehealth Into Core Workflows
Rather than expanding telehealth usage broadly, the provider focused on specific workflow points where virtual interactions could replace or enhance existing processes.
Key integration steps included:
- Using telehealth for intake qualification and education
- Conducting virtual follow-ups to confirm equipment use and address questions
- Capturing documentation in real time during virtual visits
- Aligning telehealth scheduling with billing and authorization milestones
Staff received targeted training to ensure telehealth interactions supported documentation and compliance requirements rather than operating separately.
Operational Impact: Measurable Efficiency Gains
Within six months of implementation, the provider observed clear operational improvements.
Results included:
- A 30% reduction in intake cycle time, driven by faster qualification and fewer follow-ups
- Fewer missed appointments, as virtual visits reduced travel and scheduling barriers
- Decreased documentation rework, with information captured accurately at the point of interaction
By compressing workflows rather than adding steps, telehealth reduced administrative burden instead of shifting it.
Revenue-Cycle and Compliance Outcomes
Importantly, efficiency gains did not come at the expense of compliance.
The provider aligned telehealth documentation with existing billing standards and maintained clear audit trails. Documentation captured during virtual visits supported medical necessity and delivery records, aligning with requirements under 42 CFR § 424.57.
As a result:
- Billing delays decreased
- Denial rates tied to documentation gaps declined
- Audit readiness improved
Telehealth strengthened—not weakened—defensibility.
Patient Experience Improvements
Patient feedback highlighted benefits beyond efficiency.
Patients reported:
- Greater convenience and flexibility
- Clearer understanding of equipment use
- Faster resolution of questions and issues
Satisfaction scores improved, particularly among patients with mobility limitations or transportation challenges. Telehealth enhanced engagement without replacing necessary in-person care.
Lessons Learned From the Integration
The provider identified several lessons applicable to other DME organizations:
- Telehealth works best when tied to specific workflow objectives
- Documentation capture must be integrated, not retroactive
- Staff training is essential to consistency
- Governance ensures telehealth supports compliance
Technology alone was not the differentiator—process alignment was.
How Wonder Worth Solutions Supported the Initiative
Wonder Worth Solutions worked with the provider to identify where telehealth could deliver the greatest operational impact, align virtual workflows with billing and compliance requirements, and establish governance to sustain results.
The focus was integration, not expansion.
Conclusion
This case study demonstrates that telehealth can be a powerful operational tool for DME providers when implemented intentionally. By embedding virtual interactions into intake, documentation, and follow-up workflows, the provider achieved meaningful efficiency gains, improved patient experience, and maintained compliance integrity.
Telehealth succeeded not because it was adopted—but because it was integrated.