Answer Summary
Advanced denial management for DME providers focuses on transitioning from a reactive “appeal-everything” mindset to a structural prevention model that identifies and resolves root-cause workflow failures. This evolution is critical as 2026 industry data shows a 25% surge in first-pass denials driven by AI-powered payer audits, making manual intervention alone insufficient for recovery. By prioritizing high-value claims and implementing standardized appeal playbooks, providers can effectively lower their denial rates while stabilizing their long-term cash flow.
Introduction: Why Denial Management Must Evolve Beyond Appeals
For many DME providers, denial management still revolves around a familiar rhythm: receive the denial, correct the issue, submit an appeal, and wait. While this approach addresses individual claims, it does little to reduce overall denial volume or stabilize cash flow.
By 2026, this reactive model is no longer sustainable.
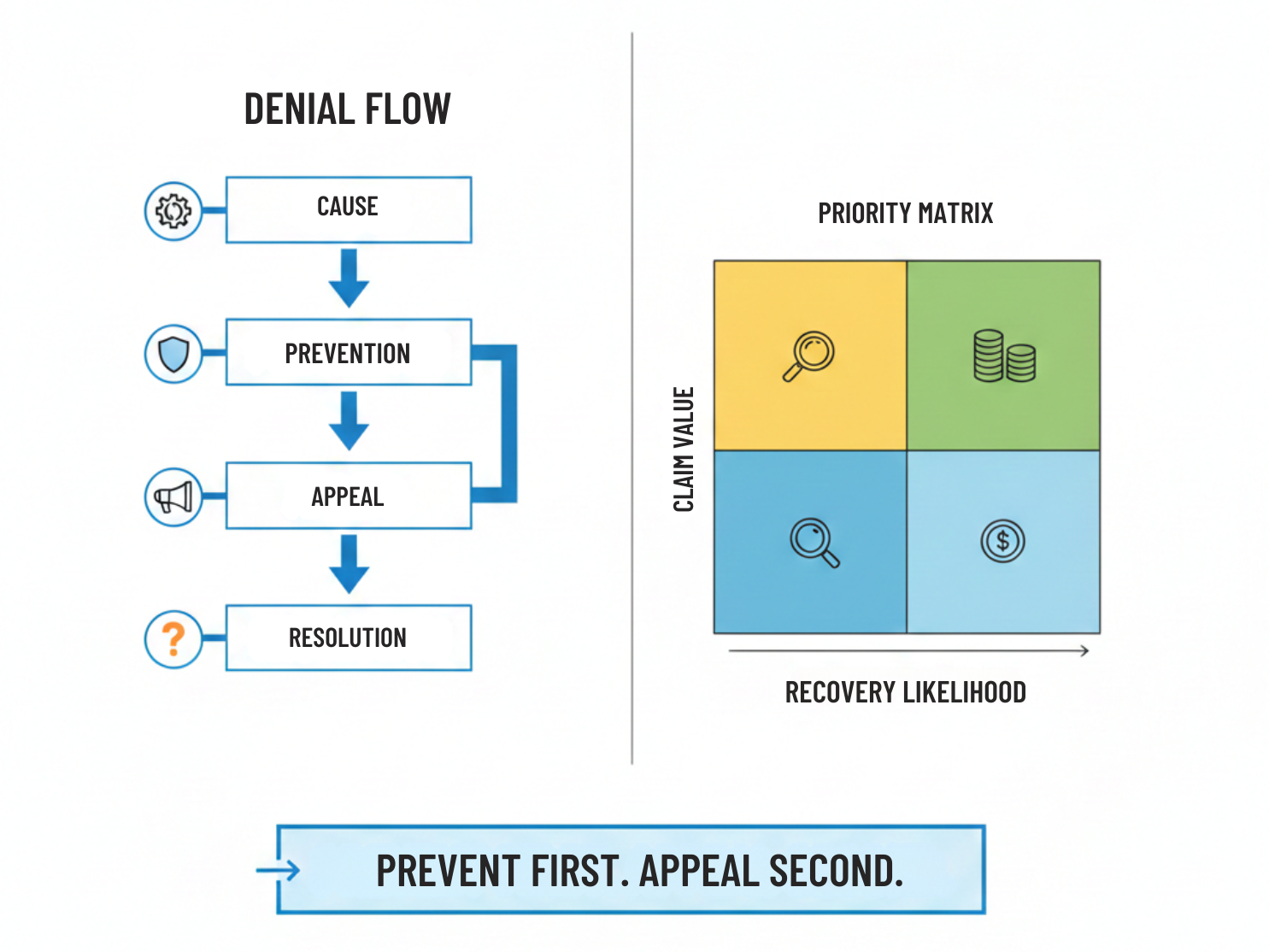
Denials are arriving faster, in greater volume, and with less tolerance for correction. Appeals are taking longer, recovery rates are tightening, and payer behavior is increasingly automated. Advanced denial management is therefore not about appealing more efficiently—it is about preventing avoidable denials, prioritizing effort intelligently, and appealing strategically.
This rapid solver focuses on how DME providers can modernize denial management without adding unnecessary complexity.
Step One: Separate Preventable Denials From Unavoidable Ones
Not all denials deserve equal attention.
The first step in advanced denial management is segmentation. Providers should classify denials into clear categories:
- Preventable denials (documentation gaps, authorization issues, intake errors)
- Contested denials (medical necessity disputes, payer interpretation differences)
- Administrative denials (timing, formatting, eligibility lapses)
Preventable denials signal workflow failures. Appealing them repeatedly without fixing root causes wastes resources. Advanced denial management focuses on eliminating recurrence, not just winning appeals.
Step Two: Link Denials Back to Workflow Stages
Denials do not originate in the billing department. They are the downstream result of upstream breakdowns.
Effective providers map denial reasons back to specific workflow stages:
- Intake
- Documentation collection
- Authorization
- Delivery
- Claim submission
This mapping reveals patterns that are invisible when denials are reviewed in isolation. Repeated documentation-related denials, for example, often point to intake inconsistency rather than billing error.
Closing this loop is essential to reducing future denial volume.
Step Three: Prioritize Denials Based on Financial and Recovery Impact
Traditional denial queues often sort by date received or aging. This approach assumes all denials are equally recoverable.
Advanced denial management uses prioritization criteria such as:
- Dollar value of the claim
- Likelihood of successful appeal
- Time sensitivity
- Payer-specific recovery patterns
By focusing human effort where recovery is most likely and impactful, providers improve cash flow without increasing staff workload.
Step Four: Standardize Appeal Playbooks by Denial Type
Appeals are often handled inconsistently, depending on staff experience or time pressure. This variability reduces effectiveness.
High-performing providers develop appeal playbooks that define:
- Required documentation for each denial type
- Standard language aligned with payer expectations
- Escalation paths when first-level appeals fail
Standardization improves appeal quality and reduces rework. It also allows newer staff to contribute effectively without extensive trial-and-error.
Step Five: Use Denial Data as a Preventive Tool
Denial data is one of the most underutilized assets in DME operations.
Providers should analyze denial trends by:
- Payer
- Product category
- Location
- Staff role
- Documentation type
These insights should feed back into training, workflow design, and intake requirements. When denial data informs prevention, appeal volume declines naturally.
Step Six: Align Denial Management With Compliance Discipline
Denial resolution must operate within compliance boundaries. Shortcuts taken to win appeals can create audit exposure later.
Under 42 CFR § 424.57, suppliers are responsible for maintaining documentation that substantiates services billed. Appeals should strengthen defensibility, not introduce risk.
Providers should ensure:
- Appeals rely on complete and accurate records
- Corrections are documented consistently
- Patterns of denial do not signal systemic noncompliance
Advanced denial management balances recovery with compliance integrity.
Step Seven: Measure Denial Management Effectiveness Correctly
Denial performance is often measured by appeal volume or win rate alone. These metrics are incomplete.
More meaningful indicators include:
- Reduction in repeat denial types
- Time to resolution by denial category
- Staff effort per recovered dollar
- Denial prevention rate over time
These metrics reveal whether denial management is improving system reliability or simply keeping pace with volume.
Common Advanced Denial Management Mistakes
Providers often struggle when they:
- Treat all denials as appeal opportunities
- Fail to address root causes
- Over-prioritize low-recovery claims
- Allow inconsistent appeal practices
Advanced denial management requires discipline and focus—not more activity.
How Wonder Worth Solutions Helps
Wonder Worth Solutions helps DME providers modernize denial management by identifying root causes, designing prioritization frameworks, and aligning appeal strategies with compliance requirements. The result is lower denial volume, improved recovery efficiency, and more predictable revenue performance.
Conclusion
In 2026, effective denial management is no longer defined by how many appeals are filed. It is defined by how many denials are prevented, how intelligently effort is prioritized, and how defensible recovery actions remain. DME providers that adopt advanced denial management practices reduce operational drag and protect cash flow in an increasingly automated payer environment.

